
Data sources and survey populations
This analysis combines data from 3 STEPs surveys in Vietnam. The sample size, sampling method, and study subjects (i.e., ages 18 to 69) were similar for STEP 2015 and 2021. Both recent rounds applied two-stage random systematic sampling methods (i.e. the primary sampling unit was Enumeration Areas) with a sampling frame consisting of 15% of the population of Vietnam and representing all 63 provinces and cities. In STEPs 2015, the final sample sizes for STEPs 1, 2 and 3 were 3,758 (97.4% response rate), 3,036 (78.7% response rate) and 2,816, respectively. (response rate of 73.0%). In STEPs 2021, the sample size included 4,738 subjects in STEP1 (94.76% response rate) and 3,712 subjects in STEPs 2 and 3 (74.2% response rate). The 2010 survey applied a three-stage sampling method and collected data from only 8 provinces, representing 8 ecological regions of Vietnam.
The random sampling method was applied as follows. In the first stage, using the main sampling frame of the General Bureau of Statistics of Vietnam, two stratifications were created: (1 = urban; 2 = rural, and within each group divided into 3 subgroups: coastal, plain and mountainous, which gives 6 strata). In each stratum, primary sampling unit (PSU) sampling applied the probability proportional to size (PPS) sampling method to select the required number of enumeration areas (EAs) in that stratum. During the second stage of sampling, households in each selected EA were randomly selected from the EA sampling frame. Subsequently, an eligible person was randomly selected from each household chosen for the STEPS 1 interview. The selection of this person is automatically executed by the Android tablet program once the eligible household members have entered the Android tablet.
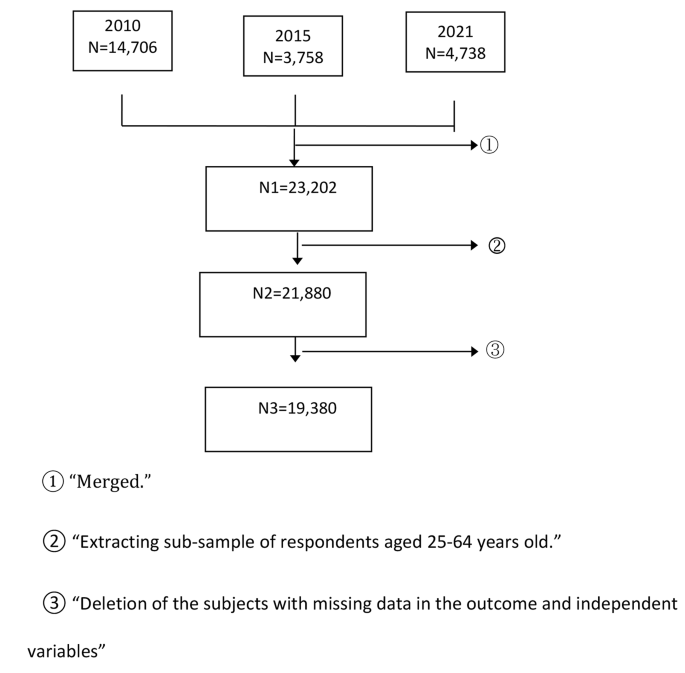
Study subjects in this cycle only include people aged 25 to 64. The sample size of the 2010 STEPS survey was 14,706 people. Panel data for 3 waves of STEPs were constructed in this study. As the subject age selection criteria differed across the three stages, we selected the data for the population aged 25–64 years. Figure 1 shows the derivation of study samples from datasets. After applying exclusion criteria, the study samples included 19,380 observations for analyses.
Derivation of the study sample
Key Metric
Study results
Hypertension
defined as an average of three measured systolic blood pressures (SBP) ≥ 140 mmHg and/or an average of three measured diastolic blood pressures (DBP) ≥ 90 mmHg, and/or previous self-reported diagnoses of hypertension by a healthcare professional , and/or self-reported current treatment for hypertension with antihypertensive medications in the previous 2 weeks (13).
Diabetes
defined as a measured blood glucose (plasma-venous value) ≥7 mmol and/or who was currently taking medication for diabetes (13).
Comorbidity of hypertension and diabetes
a person suffering from both hypertension and diabetes.
Independent variables
age range
A categorical variable with 4 classes, 25 to 34 years old, 35 to 44 years old, 45 to 54 years old and 55 to 64 years old.
Geographical area
a binary variable (1 for urban and 2 for rural).
High body mass index (BMI)
BMI was calculated as weight (kg)/height2 (m). High BMI was defined as a subject with a BMI score equal to or greater than 25.
Group behavioral risk factors
A categorical variable (ranging from 0 to 4) combining 4 behavioral risk factors for NCDs (i.e., current smoking, current alcohol consumption, not meeting physical activity levels recommended by the World Health Organization (WHO) and insufficient consumption of vegetables/fruits per day. The 4 NCD risk factors were defined as follows: (1) Current smoking: Respondents were asked the question: “Do you currently smoke tobacco daily, less than daily, or not at all?” » and were defined as current smokers if participants chose to currently smoke tobacco daily or less daily; (2) Current drinker: respondents were defined as current drinkers if they consumed at least one standard drink of alcohol in the past 30 days; (3) Not enough physical activity (PA): The WHO recommendation on PA for health was: “throughout a week, including work-related activities, during transportation and leisure, adults should do at least an equivalent combination of moderate- and vigorous-intensity physical activities. activity reaching at least 600 task metabolic equivalents (MET)-minutes”, so that a person with a total PA score in MET less than 600 MET-minutes in this study was defined as “not meeting the task recommendations ‘WHO’; (4) Not eating enough fruits/vegetables: Consume less than 5 servings of fruits/vegetables per typical day.
Statistical approach
The STATA 18 SVY procedure was used to estimate the overall prevalence of hypertension, diabetes, comorbidities and their 95% CI for the years 2010, 2015 and 2021. Survey weights were used for all calculations. Trends in T2DM-HTN comorbidity across age, gender, and geographic subgroups were also estimated. Multiple logistic regression was applied to examine factors correlated with T2DM-HTN comorbidity outcomes. Independent variables examined in the model included survey year, age group, sex, location, BMI score, and number of NCD behavioral risk factors. Variables to be included in the multivariate model were chosen using two criteria: either a p-value of the bivariate association with outcomes < 0.2, or the variables were judged to be of biological importance (e.g., sex) . Two modeling strategies — input (i.e., include all model variables simultaneously) and stepwise (i.e., iteratively add or remove potential explanatory variables and test for statistical significance after each iteration) — were evaluated. Both models produced identical results; therefore, the results of the model using the enter method were reported. A p-a value <0.05 was considered statistically significant.
As the outcome focused on T2DM-HTN comorbidity, inclusion of individuals with a single disease (i.e. T2DM or HTN) in the comparison group could potentially impact the strength of the association between NCD behavioral risk factors and outcome. Therefore, a sensitivity analysis was carried out, comparing two models:
-
Model (1) used the entire data set, the outcome of which was comorbidity, and all individuals with only one status (diabetes or hypertension) were placed in the no outcome group (sample size = 19,380 topics).
-
Model (2) used data exclusively from individuals with comorbidity and those with neither hypertension nor diabetes (individuals with either disease were excluded from the analysis, size of the sample = 14,941 subjects).
Both models revealed the same significant predictors, with the odds ratios (OR) being slightly higher in the second model. However, because the objective of the study was to identify correlated factors of comorbidity, the results of the first model were reported. We also checked for autocorrelation in the result of a final regression model with the Durbin-Watson (DW) test, the DW statistic was equal to 1.79, indicating zero autocorrelation.
Ethical consideration
The paper was based on secondary data from STEPS 2010, 2015 and 2021, with all identifying information removed. All procedures performed in WWTPs involving human participants were in accordance with the ethical standards of the Biomedical Research Ethics Review Board. The original STEPS surveys were approved by the Ethics Committee of the Vietnamese Ministry of Health and the Tasmanian Health and Human Medical Research Ethics Committee in 2010 and by the Hanoi School of Public Health in 2015 and 2020. All information on the original dataset was collected confidentially.